Abstract
The global prevalence of diabetes is predicted to increase dramatically in the coming decades as the population grows and ages, in parallel with the rising burden of overweight and obesity, in both developed and developing countries. Cardiovascular disease represents the principal cause of death and morbidity among people with diabetes, especially in those with type 2 diabetes mellitus. Adults with diabetes have 2–4 times increased cardiovascular risk compared with adults without diabetes, and the risk rises with worsening glycaemic control. Diabetes has been associated with 75% increase in mortality rate in adults, and cardiovascular disease accounts for a large part of the excess mortality. Diabetes-related macrovascular and microvascular complications, including coronary heart disease, cerebrovascular disease, heart failure, peripheral vascular disease, chronic renal disease, diabetic retinopathy and cardiovascular autonomic neuropathy are responsible for the impaired quality of life, disability and premature death associated with diabetes. Given the substantial clinical impact of diabetes as a cardiovascular risk factor, there has been a growing focus on diabetes-related complications. While some population-based studies suggest that the epidemiology of such complications is changing and that rates of all-cause and cardiovascular mortality among individuals with diabetes are decreasing in high-income countries, the economic and social burden of diabetes is expected to rise due to changing demographics and lifestyle especially in middle- and low-income countries. In this review we outline data from population-based studies on recent and long-term trends in diabetes-related complications.
Introduction
Diabetes is a major cause of morbidity and mortality worldwide and it contributes substantially to healthcare costs. In 2017 diabetes accounted for 425 million cases and its prevalence will rise to 629 million by 2040.1 Type 2 Diabetes mellitus (T2DM) is the most common type of diabetes, accounting for approximately 90% of all cases.1 A global increase of unhealthy lifestyle, the aging of the population and the escalating rates of obesity among adults and children can partially explain the diabetes pandemic. Moreover, as a result of economic development and urbanization, the incidence of diabetes is rapidly increasing in the developing countries. In addition, enhanced recognition and improved management of patients with T2DM increases longevity, further increasing the diabetes population.2 A substantial portion of diabetes health burden can be attributed to diabetes related macrovascular and microvascular complications such as coronary heart disease (CHD), stroke, peripheral artery disease (PAD), heart failure (HF), diabetic retinopathy (DR), renal disease and cardiac autonomic neuropathy (CAN) (Figure 1). Cardiovascular disease (CVD) represents the main cause of morbidity and mortality in subjects with T2DM3 in whom it occurs approximately 15 years earlier than in people without diabetes4 and it is more common in women, who show a mortality rate from CVD higher than men when compared with the counterpart without diabetes (2–5 times vs 1–3 times).5,6 Proper control and treatment of diabetes is therefore crucial as the prevalence of the disease continue to mount. This review provides an overview of worldwide trends of diabetes-related cardiovascular complications, focusing on population-based studies.
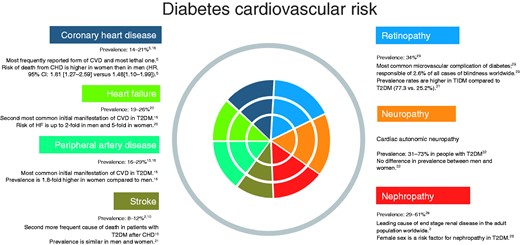
Overview of diabetes cardiovascular complications and related trends.
CHD: coronary heart disease; CI: confidence interval; CVD cardiovascular disease; T1DM: type 1 diabetes mellitus; T2DM: type 2 diabetes mellitus.
{kind=link}
Diabetes-related cardiovascular complications
It is important to adequately manage diabetes as a CVD risk factor, since the early stages of vascular complications may already be present before diagnosis or associated with pre-diabetes stages. Fasting plasma glucose (FPG) has been reported to be linearly and significantly associated with risk of CVD at all concentrations, including below the threshold for diabetes (7 mmol/l = 126 mg/dl) and increasing glycaemia influences the prognosis negatively starting from FPG concentrations of 5.6 mmol/l ( = 101 mg/dl).7 Data from the international prospective EpiDREAM cohort study concluded that the risk of CVD increased progressively among normoglycaemic individuals, people with impaired fasting glucose (IFG) or impaired glucose tolerance (IGT) and newly diagnosed diabetes subjects: a 1 mmol/l increase in FPG was associated with a 17% increase in the risk of future cardiovascular events or death.8 Additionally, dysglycaemia is a strong risk factor especially in some groups of subjects at lower CVD absolute risk such as younger ages and non-smokers.7 Overall, these data suggest that approaching dysglycaemia as a continuous risk factor, as in the case of blood cholesterol and blood pressure (BP), might represent a more effective preventive strategy for cardiovascular risk assessment and prevention than focusing on specific cutoffs. Different pathophysiological mechanisms underlie the relationship between diabetes and CVD. Abundant epidemiological data support the pathophysiological role of hyperglycaemia, as it exerts a direct effect on endothelial function and on the induction and progression of atherosclerosis,3 but other pathophysiologic factors such as hyperinsulinaemia, insulin resistance and dyslipidaemia are involved.9 Hyperinsulinaemia activates multiple inflammatory signalling pathways that promote the development and progression of atherosclerosis whereas dyslipidaemia causes mitochondrial dysfunction and consequent cell death.3.9 These mechanisms are responsible for cardiac and vasculature injury and represent common pathways for the development of both macro and microvascular complications.
Macrovascular complications
Arteriosclerotic cardiovascular diseases (ASCVDs) such as CHD, PAD and stroke are all common among people with diabetes, and their prevalence increases with worsening glucose status because of a higher risk of accelerated atherosclerosis and other more direct lipotoxic and glucotoxic effects. Concomitant risk factors such as smoking, arterial hypertension, obesity and dyslipidaemia further increase the likelihood of these complications.
CHD
In a recent systematic review of 4,549,481 individuals with T2DM, with an overall prevalence of macrovascular complications of 32.2%, CHD was the most frequently reported form of CVD (21.2%).10 After sudden cardiac death, which represents the largest subcategory of cardiovascular death in subjects with T2DM and established ASCVD (27% of cardiovascular deaths), acute myocardial infarction (MI), along with stroke, represents the second most lethal complication (21%).11 Several follow-up studies came to the similar conclusion that T2DM is a CHD ‘equivalent’, as T2DM without any prior evidence of CHD indicates a similar or higher risk of CHD than prior evidence of CHD, especially in women.12 In people with diabetes, CHD is often detected at more advanced stages of the disease in comparison with the overall population because they might experience ‘silent’ ischaemia. It has been demonstrated that even among people with diabetes without clinically established CHD, almost 75% had high-grade coronary atherosclerosis, proving that in people with diabetes the arteriosclerotic process develops faster, earlier, and is more widely spread.13 Despite improvements in cardiac care, diabetes still doubles the risk of mortality from MI, particularly in women: a three-year retrospective cohort study on 407,161 subjects found an incidence rate of death from MI of 1.81 in female (95% confidence interval (CI): 1.27–2.59) vs 1.48 in men (95% CI: 1.10–1.99).5 Lipid levels, together with systolic BP and smoking, are significant predictors of CHD risk and mortality in diabetes. Data on participants from the Atherosclerosis Risk in Communities Study and from the Reasons for Geographic and Racial Differences in Stroke Study indicated lipid-lowering medication use and lower low-density lipoprotein (LDL)-cholesterol as factors accountable for 33.6% (95% CI: 0.4–91.9%) and 27.2% (95% CI: −2.9−67.6%) of the observed decline in CHD incidence and mortality in people with diabetes.14
Peripheral artery disease
PAD is the atherosclerotic occlusive disease of lower extremity arteries and is associated with ASCVD of other vascular beds, including the cardiovascular and cerebrovascular systems. PAD in diabetes often involves more distal vessel segments in the cruro-pedal region as compared with people without diabetes and may be accompanied by medial sclerosis of the Mönckeberg type, with both factors contributing to extra therapeutic and diagnostic difficulties.6 PAD frequently manifests itself with claudication, but it can culminate with lower extremity amputation. A systematic review including 112,027 participants from high and low-income countries estimated an increase of 23.5% in the decade between 2000–2010 in the number of people living with PAD,15 and presently it is the most common initial manifestation of CVD in T2DM.16 In a recent cohort study on 1.9 m people with diabetes, 16.2% of patients presented with PAD as the first cardiovascular presentation.16 Women showed higher rates of PAD compared with men, especially in low and middle-income countries, with an estimated prevalence of ankle-brachial index ≤1.0 of 26.6% vs 14.4%.6 The outcome of patients with PAD depends on concomitant complications, advanced age, smoking and glycaemic control. Altered metabolism has been associated with a greater need for lower extremity bypass surgery and amputation and with a worse outcome following vascular surgery.17 In a single-centre retrospective study on diabetes patients undergoing infrapopliteal angioplasty, at one-year follow-up freedom from restenosis or reintervention was 16% for patients with pre-procedure FPG values above the median and 46% for patients with below the median FPG values.17
Stroke
Diabetes-related stroke is the consequence of extracranial carotid artery disease and intracranial large and small vessel diseases induced by diabetes, and the clinical manifestations range from asymptomatic carotid artery occlusion or cerebral small vessel disease to transitory ischemic attack and to haemorrhagic and ischaemic stroke. Diabetes is an independent risk factor for stroke with an incidence 2.5–3.5 times higher than in individuals without diabetes, and stroke is the most frequent cause of death in patients with T2DM after CHD.10 Furthermore, hospitalization for stroke is longer and the neurological sequelae are more severe in the diabetes population compared with the population without diabetes.18 Inadequate glycaemic control increases the risk of death from stroke: for every 1% rise in haemoglobin A1c (HbA1c) the possibility of stroke-related death is 1.37 higher.16 On the other hand, hypertensive management has been shown to reduce the incidence of stroke in people with diabetes in several randomised trials. In particular, a treatment with angiotensin-converting enzyme inhibitors (ACEIs) demonstrated a reduction in stroke risk of 33% in 3577 high-risk diabetes subjects from the Heart Outcomes Prevention Evaluation study, whereas in the Perindopril Protection Against Recurrent Stroke Study study the diabetes patients treated with ACEIs gained the same benefit from active treatment as those without.18
Cardiomyopathy due to diabetes and HF
Although commonly referred to as a diabetes-related macrovascular complication, cardiomyopathy due to diabetes and HF results from a more complex pathophysiology, which also includes microvascular dysfunction and metabolic disorders. Diabetes induces changes in the myocardium including metabolic, structural and functional alterations, which, in the absence of concomitant cardiac diseases, fall under the definition of diabetes mellitus-induced cardiomyopathy (DMCMP). DMCMP is imputable to long-standing hyperglycaemia and consequent oxidative stress and manifests itself with different clinical and echocardiographic phenotypes: (a) men with preserved systolic and diastolic function; (b) obese and hypertensive women with diastolic dysfunction; (c) men with left ventricular (LV) hypertrophy and systolic dysfunction.9,19 Initial subclinical cardiac abnormalities of DMCMP, such as LV fibrosis and increased LV stiffness, might occur independently of diabetes duration and quality of metabolic control and can progress to symptomatic HF.9,20 In diabetes clinical trials, subjects with HF are poorly represented and therefore the prevalence of HF in diabetes is underestimated, ranging from 19–26%.20 Data from The Framingham Heart Study suggest that the risk of HF is higher in women than in men with diabetes (up to five-fold in women vs two-fold in men) compared with age-matched controls.20,21 HF is a major cause of hospitalization in diabetes, and both hospitalization and mortality from HF do not seem to be preventable by tight glycaemic control, especially with older drugs such as sulphonylureas, metformin, thiazolidindiones and insulin, suggesting that additional factors beyond glycaemia might contribute to the increased HF risk in diabetes. Indeed, a meta-analysis on 37,229 patients showed no effect of intensive glycaemic control on the risk of HF in patients with T2DM, with an odds ratio of 1.20 (95% CI: 0.96–1.48) between intensive and standard glycaemic control.22 In a cohort study on 271,174 people with T2DM from the Swedish National Diabetes Register and 1,355,870 matched controls, the risk of hospitalization for HF was the highest in people with T2DM who were younger than 55 years of age and with several risk factors (HbA1c, LDL-cholesterol, BP, albuminuria and smoking) outside the target (hazard ratio (HR) vs controls, 95% CI: 11.35 (7.16–18.01)). The presence of atrial fibrillation, a high body mass index (BMI) and a HbA1c and renal function outside the target were the strongest predictors of hospitalization for HF.23 Finally, HF in diabetes might occur as HF with reduced ejection fraction (HFrEF) or preserved ejection fraction (HFpEF). Along with the increasing prevalence of HFpEF relative to HFrEF, a growing relevance is attributed to T2DM as a key factor in the pathophysiology of LV diastolic dysfunction, and HFpEF nowadays represents the most common type of HF in T2DM.9,19
Microvascular complications
Diabetes microvascular complications account for a substantial increase in morbidity and a considerable impairment in the quality of life in people with diabetes. Microvascular complications of diabetes are principally nephropathy, retinopathy and CAN.
Nephropathy
Nephropathy is defined by elevated urine albumin excretion and chronic kidney disease (CKD) by reduced glomerular filtration rate (GFR) and occurs as consequence of long-term inadequate glycaemic control. Nowadays renal disease in individuals with diabetes represents the largest group with end-stage renal disease in the adult population worldwide. Clinically, it ranges from microalbuminuria to CKD, and the risk of progression depends on the concomitant presence of uncontrolled hypertension, dyslipidaemia, hyperglycaemia, smoking and genetic predisposition.2 Some controversy exists regarding the value of tight glycaemic control to reduce renal complications and renal death in diabetes. One recent meta-analysis, based on 16 guidelines and 328 statements, looked at hard but infrequent endpoints (need of dialysis, end-stage renal disease, renal death) and found no significant impact of tight glycaemic control (HbA1c < 6.5–7.0%) compared with less tight control (HbA1c = 7.0–8.5%).24 Another analysis, based on four large-scale randomised controlled trials, investigated wider predefined primary renal outcomes (a composite of end-stage kidney disease, renal death, development of an estimated GFR (eGFR) rate <30 ml/min/1.73 m2, or development of overt diabetic nephropathy) and confirmed a 20% reduction.25 On the other hand, studies testing an intensified multifactorial treatment26 or treatment with renal active hypoglycaemic agents (sodium–glucose cotransporter 2 inhibitors) demonstrated a reduced risk of developing nephropathy and a reduced risk of end-stage renal disease and renal death, respectively.27 The prevalence of nephropathy increases with diabetes progression: in the United Kingdom Prospective Diabetes Study (UKPDS), 7.3% of patients with T2DM had microalbuminuria at the time of diagnosis, and the prevalence increased over time to 17.3% at five years, 24.9% at 10 years and 28.0% at 15 years, while 29.0% of participants showed a decrease of GFR below 60 ml/min/1.73 m2 at the end of the follow-up period.28 The occurrence of renal disease contributes substantially to the medical burden of T2DM and to the increased cardiovascular risk, as lower GFR and albuminuria are associated with CVD and all-cause mortality.2
Diabetic Retinopathy (DR)
DR is the most common microvascular complication of diabetes, and it is responsible for approximately 10,000 new cases of blindness every year in the USA and affects almost 100 m people worldwide.29 DR is becoming an ever-increasing health burden, with estimates between 1990–2010 showing that visual impairment and blindness caused by DR increased by 64% and 27% respectively.29 This trend might be explained by the increased prevalence of diabetes and the greater longevity among those who are affected, but the epidemiology of the disease shows significant regional differences, and developing countries are contributing substantially to the increased prevalence of DR, with the regions of North Africa/Middle East, sub-Saharan Africa and South Asia showing the highest age-standardised prevalence of DR-related blindness.29 Along with the change in the epidemiology of the disease, the concept of DR has evolved too, and the American Diabetes Association (ADA) has redefined DR as a more complex neuro-vascular complication, in which retinal neurodegeneration plays an important role.30 Many systemic features of diabetes influence the occurrence of DR. Prevalence rates increase with the duration of diabetes (21.1 vs 76.3%, comparing <10 with ≥20 years), with values of HbA1c (18.0 vs 51.2%, comparing levels ≤7.0 with > 9.0%) and BP (30.8 vs 39.6%, comparing BP ≤ 140/90 or > 140/90 mm Hg).31 Glycaemic control represents an effective treatment to slow the progression of DR: a meta-analysis of four randomised trials (Action to Control Cardiovascular Risk in Diabetes, Action in Diabetes and Vascular Disease, UKPDS and Veterans Affairs Diabetes Trial) demonstrated a relative risk reduction of 13% for eye events (such as requirement for retinal photocoagulation therapy or vitrectomy) in individuals who received an intensive glucose-lowering intervention compared with those who received the standard glucose-lowering intervention.25
CAN
Diabetes is responsible of a heterogeneous group of neuropathic disorders which affects both somatic and autonomic components of the nervous system. As for other microvascular complications, the risk of developing neuropathy in people with diabetes increases with age and it is proportional to both the magnitude and duration of hyperglycaemia. CAN is defined as the impairment of cardiac autonomic control in people with diabetes following the exclusion of other causes and it results from damage to the autonomic nerve fibres that innervate the heart.32 Hyperglycaemia plays an important role in the pathogenesis of CAN, as it activates multiple pathways which result in mitochondrial dysfunction and formation of reactive oxygen species. When symptomatic, CAN manifests itself with abnormalities in heart rate control, silent ischaemia and orthostatic hypotension. The estimated prevalence of CAN varies from 17–66% in people with type 1 diabetes mellitus (T1DM) and 31–73% in people with T2DM,32 being influenced by the diagnostic method used, age and duration of diabetes. CAN is significantly associated with morbidity such as silent myocardial ischaemia, CHD, stroke, nephropathy and with a high risk of cardiac arrhythmias and sudden death.32 As for other microvascular complications of diabetes, an intensified multifactorial intervention (hyperglycaemia, dyslipidaemia, hypertension and microalbuminuria) has been demonstrated to be effective on the development of CAN in people with T2DM, reducing the risk of progression by 68%.26
Mortality burden
Mainly due to its vascular complications, diabetes is a major global cause of mortality. The International Diabetes Federation estimated that four million people died from diabetes in 2017, and diabetes accounted for 10.7% of global all-cause mortality among people between 20–79 years old.1 Globally, there are more deaths due to diabetes in women then in men (2.1 vs 1.8 m)1 and this excess risk can be mainly attributed to the higher risk of cardiovascular mortality in women.5 A number of epidemiological studies have quantified the risk of death among people with diabetes with highly varying results, but they all agreed that mortality is mainly attributable to cardiovascular causes.5,8,10,33,34 A recent systematic review of 57 articles published between 2007–2017 with 4,549,481 persons having T2DM, estimated that deaths due to CVD represented 50.3% (95% CI: 37.0–63.7%) of all deaths in subjects with T2DM.10 In the EpiDREAM study, a cohort study on 25,063 individuals at risk for diabetes, the annualised cardiovascular death event rate was 1.27/100 person-years among those with diabetes compared with 0.51/100 person-years in normoglycaemia.8 Data from several studies suggest a decline in CVD-associated mortality among people with diabetes in most high-income countries. A recent report from the National Health Interview Survey Linked Mortality files from 1985–2015 showed a decrease of 32% every 10 years of death from vascular causes among US adults with diabetes (from 11.0 (95% CI: 9.2–12.2) to 5.2 (95% CI: 4.8–5.6) per 1000 person-years).34 Another report on the US national mortality database indicated that the age-standardised mortality rates for CHD declined significantly from 2007 to 2014 (annual percentage change (APC), 95% CI: −2.8% (−3.3– –2.3%)) and then stabilised from 2014 to 2017 (APC 95% CI: −0.6% (−2.5–1.3%)).35 On the other hand, low and middle-income countries show an opposite trend: in Mexico, diabetes prevalence increased from 7% in 2006 to 8.9% in 2012 with a mortality risk ratio of 2.0 between individuals with and without diabetes.36 Similarly, prevalence of diabetes in adults aged older than 20 years in India increased from 5.5% in 1990 to 7.7% in 2016, with an increase in both crude (131%) and age-standardised (64%) death rates due to diabetes.37 In both countries this was strongly related to an increased prevalence of overweight. We can therefore conclude that CVD remains a leading worldwide cause of death in people with diabetes.3,13,36,37
Societal and healthcare costs of diabetes
Diabetes imposes a substantial burden on society both in the form of higher direct medical costs, which include hospital inpatient care, medications, outpatients visits, and indirect medical costs, such as reduced productivity at work and increased absenteeism. A recent study in Europe showed that people with diabetes compared with those without it used approximately twice the amount of healthcare resources, started their resource use earlier in life and, as they developed complications, the healthcare costs increased markedly.38 The ADA reported the total healthcare costs of diabetes in the USA for 2017 and showed a remarkable magnitude in the total direct costs of diabetes in the US, that increased by 26% from 2012 to 2017, amounting to $327 billion in 2017 including $237 billion in direct medical cost and $90 billion in lost productivity.39 Diabetes cardiovascular complications contribute substantially to the healthcare costs of diabetes; a systematic review of articles describing the costs associated with treating CVD in subjects with T2DM reported that CVD costs amounted to 20–49% of the total direct costs of treating T2DM. At the patient level, treating patients with both CVD and T2DM resulted in a cost increase of $3418–9705 /patient/year compared with treating patients with only T2DM.40
Conclusions
Diabetes is a global healthcare problem. The number of people with diabetes is increasing, and the largest increase will take place in regions of low and middle-income, as a consequence of population aging, growth and urbanization. Progress in prevention and diagnosis of diabetes complications has led to a decline in several of these complications in developed countries. However, as a consequence of an inadequate multifactorial management, people with diabetes remain at significantly higher cardiovascular risk compared with people without diabetes and CVD is a major cause of comorbidity and death among people with diabetes. Given the large burden that diabetes exerts on the healthcare systems as a driver of CVD, the identification of new strategies to monitor and control diabetes, to better characterise its complications and more accurately quantify their prevalence becomes a major clinical imperative.
Author contribution
EDC contributed to the conception and design of the work, to the acquisition, analysis, or interpretation of data for the work, drafted and critically revised the manuscript. JWJB contributed to the conception and design of the work, to the acquisition, analysis or interpretation of data for the work and critically revised the manuscript. AC, LR, MF, TBH, OS and ES contributed to design the work and critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.